
Colleagues,
As periodontists, we occasionally encounter patients whose oral presentations suggest underlying systemic disease.
This newsletter highlights manifestations of leukemia that can be easily screened for in a dental setting, and shares a recent case that underscores the importance of vigilance.
Case Presentation: AML in a Periodontitis Patient
A male patient in his 40s with no significant medical history and a recent clean bill of health from his PCP presented for evaluation.
He had achieved periodontal stability following LANAP treatment 4 years prior. After a recent cleaning with his general dentist, he developed progressive inflammation.
Initial Findings: Increased probing depths, bleeding, and bone loss compared to previous exams. The patient also exhibited increased halitosis compared to previous maintenance visits. The patient’s clinical findings indicated a periodontitis flare-up and periodontal abscesses from incomplete calculus removal during a recent dental cleaning.
Same Day Treatment Provided: LANAP retreatment and extraction of maxillary third molars.
Post-operative Course
Over the following two weeks, the patient developed:
- Multiple liver clots at surgical sites
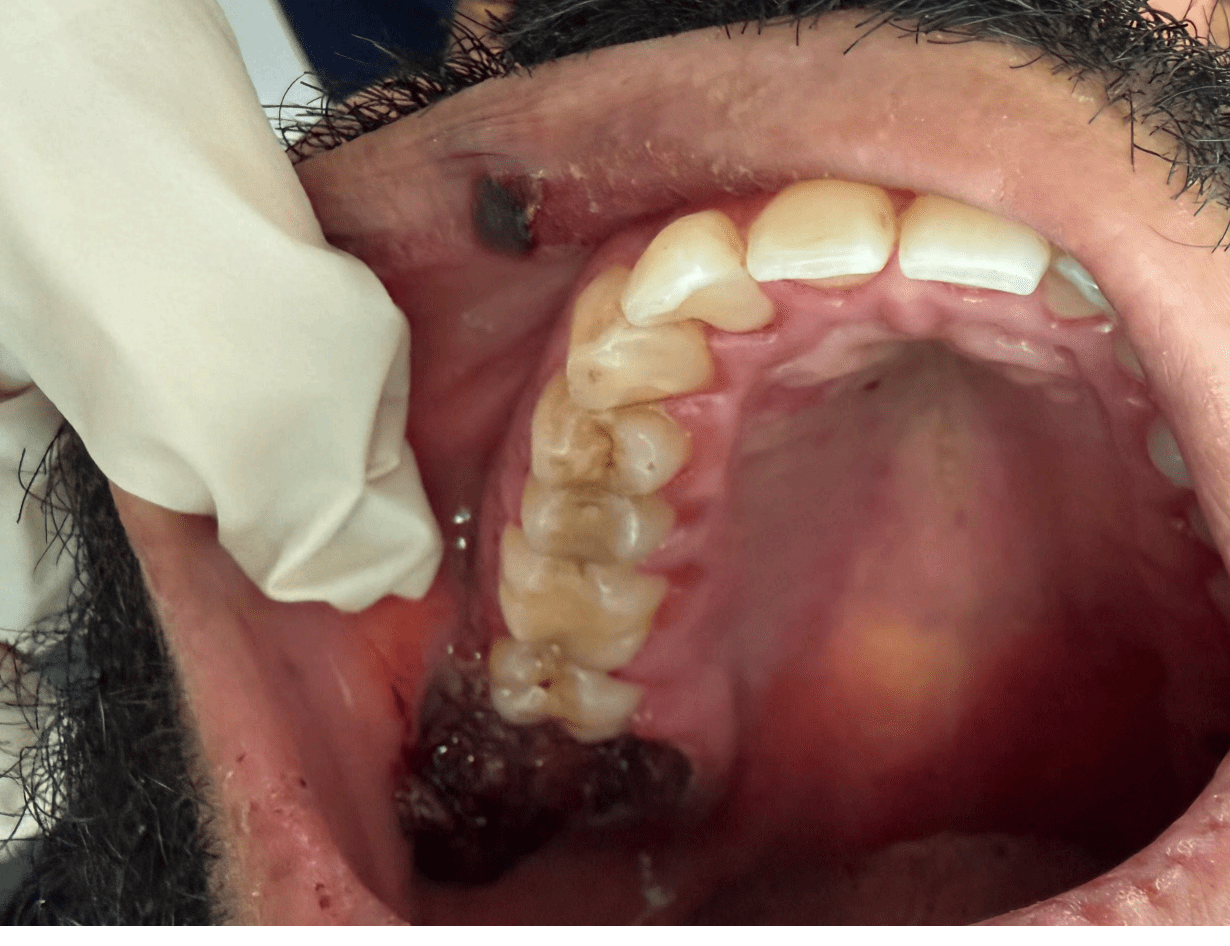
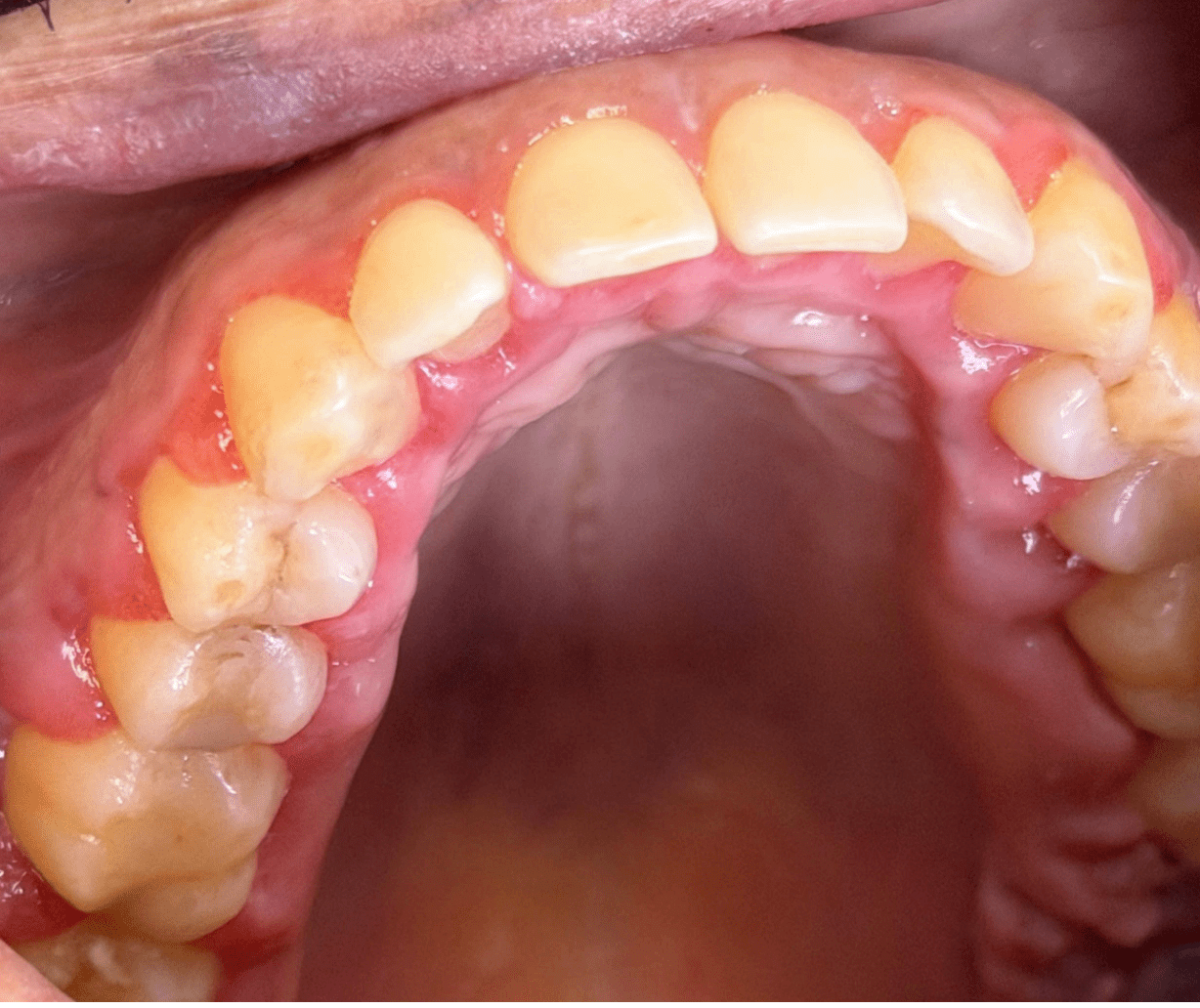
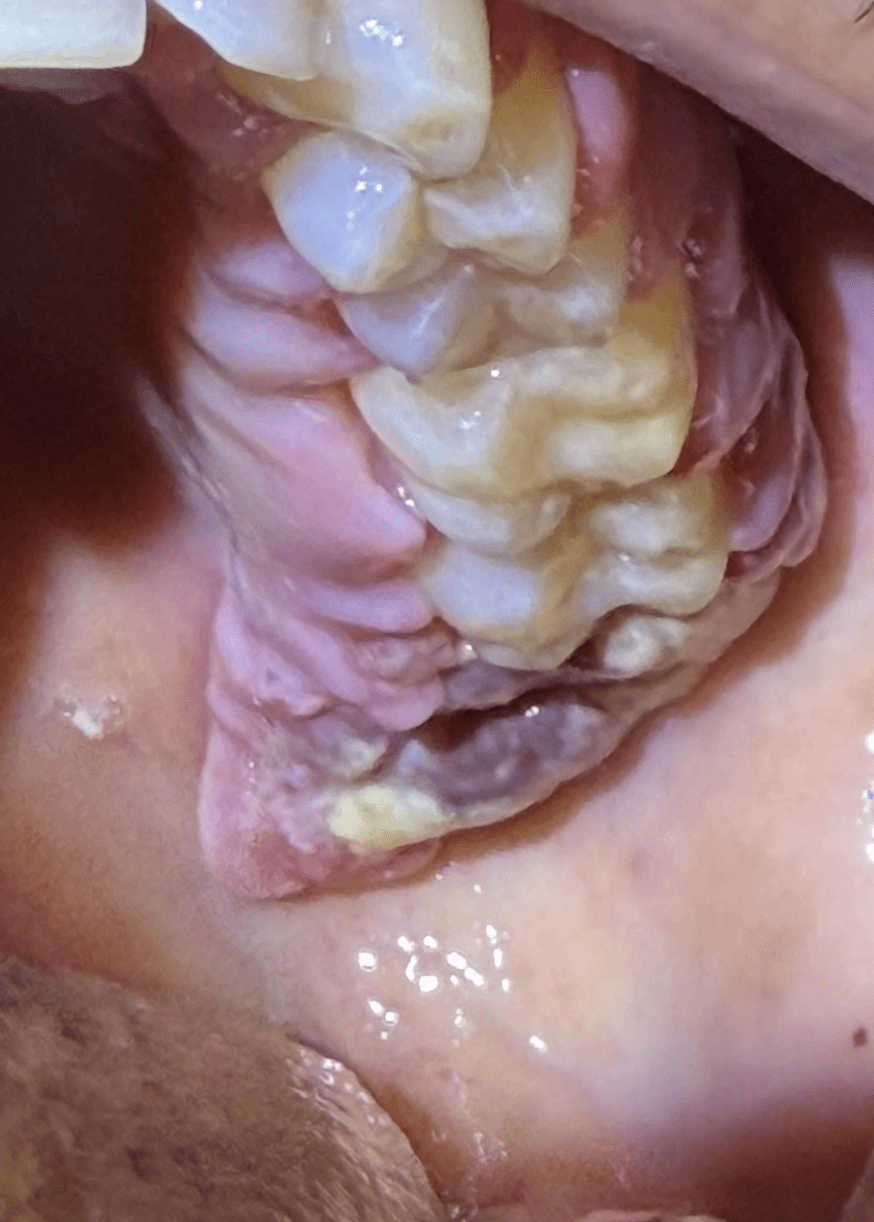
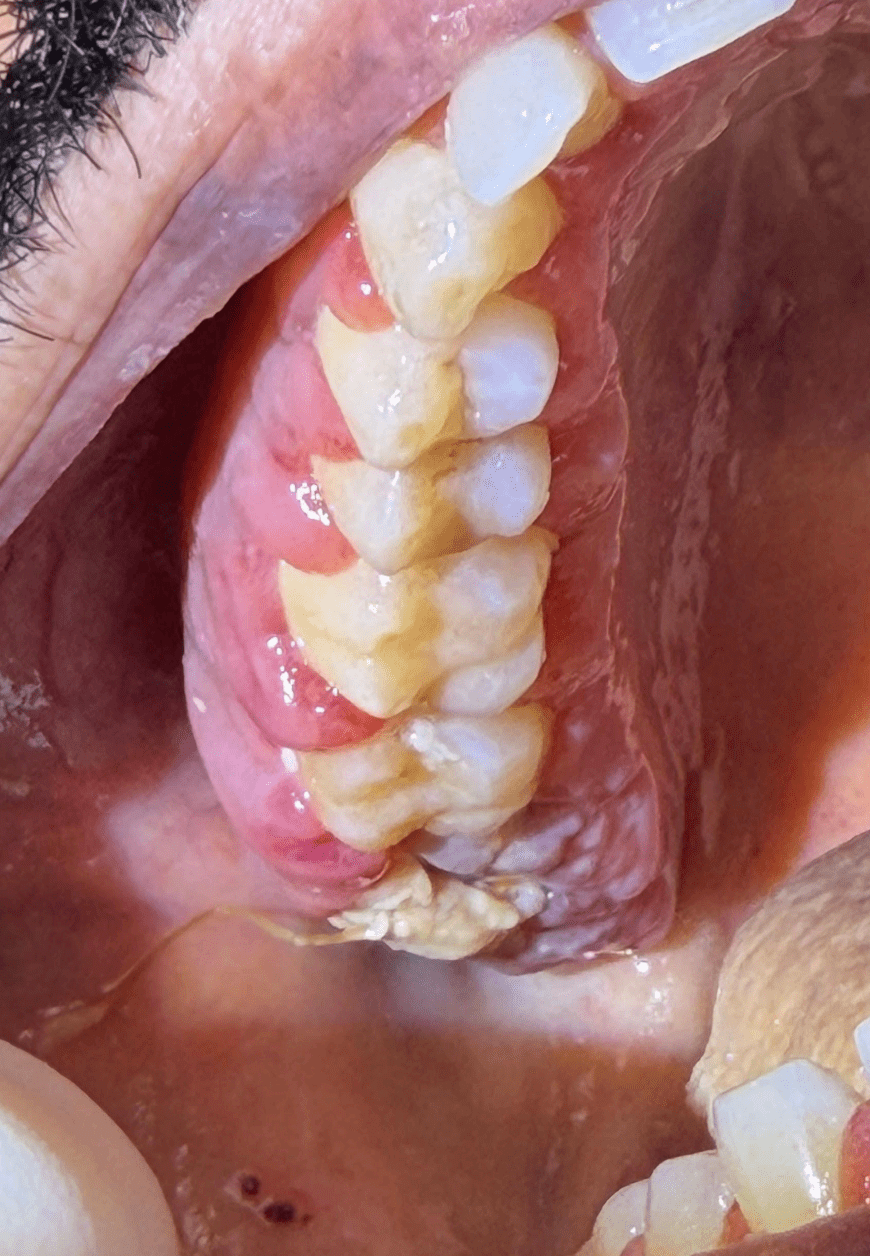
- Progressive edema and erythema of gingiva and extraction sites
- At one week: Ecchymosis and ulcerations were present intra and extraorally
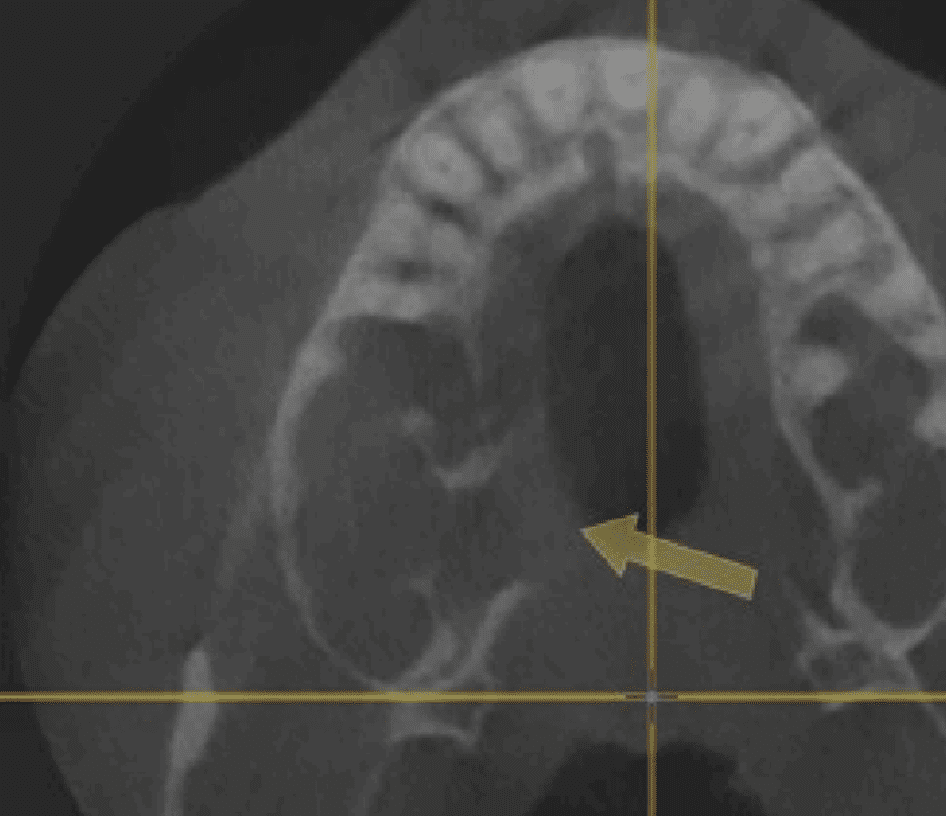
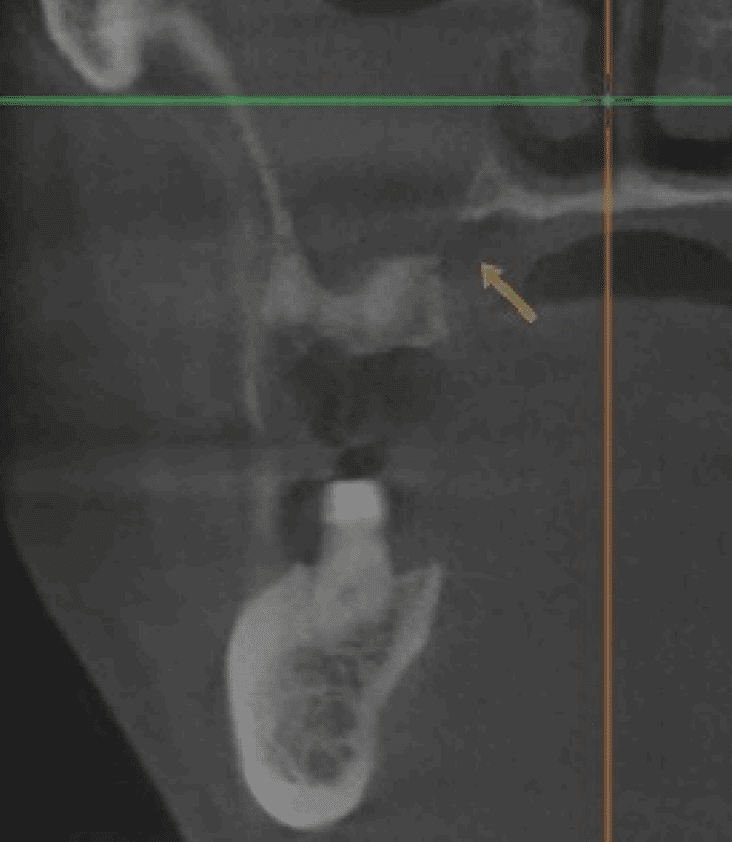
CT showed sinus opacity and cortical break in right maxillary sinus—a finding concerning for aggressive bone destruction that can indicate leukemic infiltration or pathologic bone resorption; ENT referral made.
Increased halitosis leading to suspicion of anaerobic bacterial involvement. Augmentin and metronidazole were prescribed.
At two weeks: Halitosis was no longer present following antibiotics, but delayed wound healing persisted, and further increased erythema and edema were present throughout treated areas. Patient had been unable to see ENT up to this point.
Outcome: Patient was sent to the emergency department for immediate evaluation, where he was diagnosed with acute myeloid leukemia.
Oral Manifestations of Leukemia
Oral signs occur in approximately 30% of patients with newly diagnosed acute leukemia, though classic findings like gingival enlargement are present in only about 6% of cases.[1][2] Key oral manifestations include:
- Gingival enlargement or hyperplasia (particularly in acute myeloid leukemia with monocytic subtypes)[3][2]
- Spontaneous gingival bleeding and mucosal bleeding[4][2]
- Petechiae and ecchymoses of the oral mucosa[4][2][5]
- Oral ulcerations and mucosal pallor[4][2][5]
- Poor wound healing following dental procedures[5]
- Unexplained periodontal deterioration despite previous stability[6]
- Infections (candidiasis, recurrent herpes)[2][5]
- Halitosis from oral infections, necrotic tissue, or poor oral hygiene[7][8]
Radiographic Bone Findings
Leukemia can cause significant bone changes in the maxillofacial region that may be visible on dental imaging:
- Osteolytic lesions with ill-defined borders and bone destruction are the most common radiographic findings[9][10]
- Cortical bone erosion or destruction, including breaks in the cortical plate, may indicate leukemic infiltration or aggressive bone resorption[9][10][11]
- Diffuse osteopenia and loss of trabecular pattern[12][13]
- Periosteal reactions are uncommon in leukemia, which can help differentiate from infectious processes[10]
Cortical bone destruction in leukemia results from multiple mechanisms: direct leukemic cell infiltration, increased osteoclast activity mediated by cytokines (particularly TNFα and RANKL), and impaired osteoblast function.[14][15][16] When cortical breaks are identified in patients with suspected malignancy, they may represent aggressive disease requiring urgent evaluation.[9][11]
Skin Manifestations
Leukemia cutis—infiltration of leukemic cells into the skin—occurs most commonly with acute myeloid leukemia and chronic lymphocytic leukemia.[17] Presentations include:
- Papules, nodules, plaques, or purpuric lesions[17][18]
- Typically purpuric nodules in acute myeloid leukemia[3]
- Ecchymoses and petechiae from thrombocytopenia[19]
- Lesions most frequently appear on the trunk and extremities[17]
Key Takeaways
- Unexplained periodontal deterioration in previously stable patients warrants investigation
- Poor wound healing, persistent bleeding, and progressive inflammation after routine procedures should raise suspicion
- Ecchymosis and oral ulcerations developing postoperatively, especially when progressive, may indicate underlying thrombocytopenia or coagulopathy from hematologic malignancy[3][5][20]
- Cortical bone destruction on imaging, particularly when ill-defined or aggressive in appearance, should prompt consideration of malignancy
- Patients with “clean bills of health” can still harbor undiagnosed hematologic malignancies
- Early recognition and prompt referral can be life-saving
When you encounter patients with unusual gingival presentations, spontaneous bleeding, atypical responses to periodontal therapy, or concerning radiographic bone changes, consider leukemia in your differential diagnosis. We encourage you to refer patients with concerning findings for comprehensive evaluation.
Thank you for your continued partnership in patient care.
Best,
Matthew Flaherty, DDS
References
1. Prevalence of Oral Lesions in and Dental Needs of Patients With Newly Diagnosed Acute Leukemia. Watson E, Wood RE, Maxymiw WG, Schimmer AD. Journal of the American Dental Association (1939). 2018;149(6):470-480. doi:10.1016/j.adaj.2018.01.019.
2. Oral Manifestations and Complications in Childhood Acute Myeloid Leukemia. Cammarata-Scalisi F, Girardi K, Strocchio L, et al. Cancers. 2020;12(6):E1634. doi:10.3390/cancers12061634.
3. Acute Myeloid Leukaemia. DiNardo CD, Erba HP, Freeman SD, Wei AH. Lancet (London, England). 2023;401(10393):2073-2086. doi:10.1016/S0140-6736(23)00108-3.
4. Leukemic Oral Manifestations and Their Management. Francisconi CF, Caldas RJ, Oliveira Martins LJ, Fischer Rubira CM, da Silva Santos PS. Asian Pacific Journal of Cancer Prevention : APJCP. 2016;17(3):911-5. doi:10.7314/apjcp.2016.17.3.911.
5. A Patient Presenting for Dental Extraction After Completion of Chemotherapy. Hong WW, Kim IH, Hong BM, Oak S, Mupparapu M. Dental Clinics of North America. 2023;67(4):667-670. doi:10.1016/j.cden.2023.05.020.
6. Oral Manifestations of Acute Myelomonocytic Leukemia: A Case Report and Review of the Classification of Leukemias. Wu J, Fantasia JE, Kaplan R. Journal of Periodontology. 2002;73(6):664-8. doi:10.1902/jop.2002.73.6.664.
7. Severe Necrotizing Stomatitis and Osteomyelitis After Chemotherapy for Acute Leukaemia. Santos FA, Pochapski MT, Pilatti GL, et al. Australian Dental Journal. 2009;54(3):262-5. doi:10.1111/j.1834-7819.2009.01129.x.
8. Oral Manifestations During Chemotherapy for Acute Lymphoblastic Leukemia: A Case Report. Gomes MF, Kohlemann KR, Plens G, et al. Quintessence International (Berlin, Germany : 1985). 2005;36(4):307-13.
9. Leukaemic Infiltration in the Oral and Maxillofacial Region: An Update. de Sena ACVP, de Arruda JAA, Costa FPD, et al. Journal of Oral Pathology & Medicine. 2021;50(6):558-564. doi:10.1111/jop.13206.
10. Radiological Aspects of Lymphomas and Leukaemias Affecting the Jaws: A Systematic Review. Gomes NR, Lima LA, Morais-Perdigão AL, et al. Journal of Oral Pathology & Medicine. 2023;52(4):315-323. doi:10.1111/jop.13422.
11. Unusual Maxillary Osteoblastic and Osteolytic Lesions Presenting as an Initial Manifestation of Childhood Acute Myeloid Leukemia: A Case Report. Shimizu R, Ohga N, Miyakoshi M, et al. Quintessence International. 2017;48(2):149-153. doi:10.3290/j.qi.a37383.
12. Orthopaedic Manifestations of Leukemia in Children. Rogalsky RJ, Black GB, Reed MH. The Journal of Bone and Joint Surgery. American Volume. 1986;68(4):494-501.
13. Musculoskeletal Imaging Findings of Hematologic Malignancies. Navarro SM, Matcuk GR, Patel DB, et al. Radiographics. 2017;37(3):881-900. doi:10.1148/rg.2017160133.
14. B Cell Acute Lymphoblastic Leukemia Cells Mediate RANK-RANKL-dependent Bone Destruction. Rajakumar SA, Papp E, Lee KK, et al. Science Translational Medicine. 2020;12(561):eaba5942. doi:10.1126/scitranslmed.aba5942.
15. Chronic Lymphocytic Leukemia Cells Impair Osteoblastogenesis and Promote Osteoclastogenesis: Role of TNFα, IL-6 and IL-11 Cytokines. Giannoni P, Marini C, Cutrona G, et al. Haematologica. 2021;106(10):2598-2612. doi:10.3324/haematol.2019.231456.
16. Functional Activation of Osteoclast Commitment in Chronic Lymphocytic Leukaemia: A Possible Role for RANK/RANKL Pathway. Marini C, Bruno S, Fiz F, et al. Scientific Reports. 2017;7(1):14159. doi:10.1038/s41598-017-12761-1.
17. Leukemia Cutis-the Current View on Pathogenesis, Diagnosis, and Treatment. Robak E, Braun M, Robak T. Cancers. 2023;15(22):5393. doi:10.3390/cancers15225393.
18. Leukaemia Cutis: Clinical Features and Outcomes of 56 Patients. Yook HJ, Son JH, Kim YH, et al. Acta Dermato-Venereologica. 2022;102:adv00647. doi:10.2340/actadv.v102.1123.
19. Cutaneous Manifestations in Leukemia Patients. Grunwald MR, McDonnell MH, Induru R, Gerber JM. Seminars in Oncology. 2016;43(3):359-65. doi:10.1053/j.seminoncol.2016.02.020.
20. Acute Lymphocytic Leukaemia. Kantarjian H, Pui CH, Jabbour E. Lancet (London, England). 2025;406(10506):950-962. doi:10.1016/S0140-6736(25)00864-5.